Bartter Syndrome
Autosomal Recessive disorder.
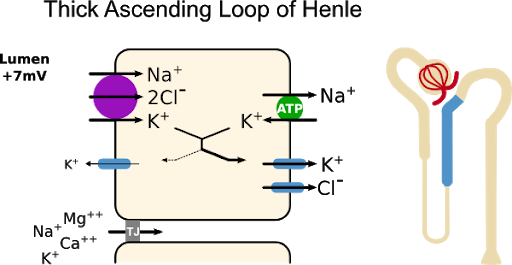
Characterized by defect in the Na-K-Cl channel in the thick ascending limb of loop of Henle
This leads to loss of Na - K - Cl into the urine.
Hypovolemia occurs which causes secondary hyperaldosteronism by activation of Renin-Angiotensinogen - Aldosterone mechanism.
This Na-K-Cl channel is responsible for creating the medullary concentration gradient that is required for excretion of maximally concentrated urine in the presence of ADH.
The impaired concentrating ability and polyuria in Bartter syndrome are mainly due to the impaired sodium transport in the loop of Henle.
High prostaglandin levels and chronic hypokalemia may also contribute.
Why metabolic alkalosis and hypokalemia in Bartter?
Volume depletion leads to secondary hyperaldosteronism; this, along with increased distal flow and delivery of sodium, results in increased urinary potassium losses and hydrogen ion secretion.
Why hypocalcemia and hypomagnesaemia in Bartter?
The paracellular reabsorption of both calcium and magnesium in the thick ascending limb requires the electrochemical gradient created by sodium chloride transport in this tubule segment. Thus, abnormal sodium chloride transport in the thick ascending limb increases renal calcium and magnesium excretion.
Hypomagnesaemia is more common in Gitlemann syndrome.
Why polyuria in Bartter syndrome?
Since Na-K-Cl is not getting absorbed the medullary concentration gradient is not established due to which large amount of fluid is lost in urine causing polyuria.
Types of Bartter syndrome




Comments
Post a Comment